
Did the Socio-Economic Gradient in Depression in Later-Life Deteriorate or Weaken during the COVID-19 Pandemic? New Evidence from England Using Path Analysis


Abstract
:1. Introduction
- (a)
- a higher chance of coronavirus infection,
- (b)
- greater difficulties in access to social services and
- (c)
- reduced social contact.
2. Materials and Methods
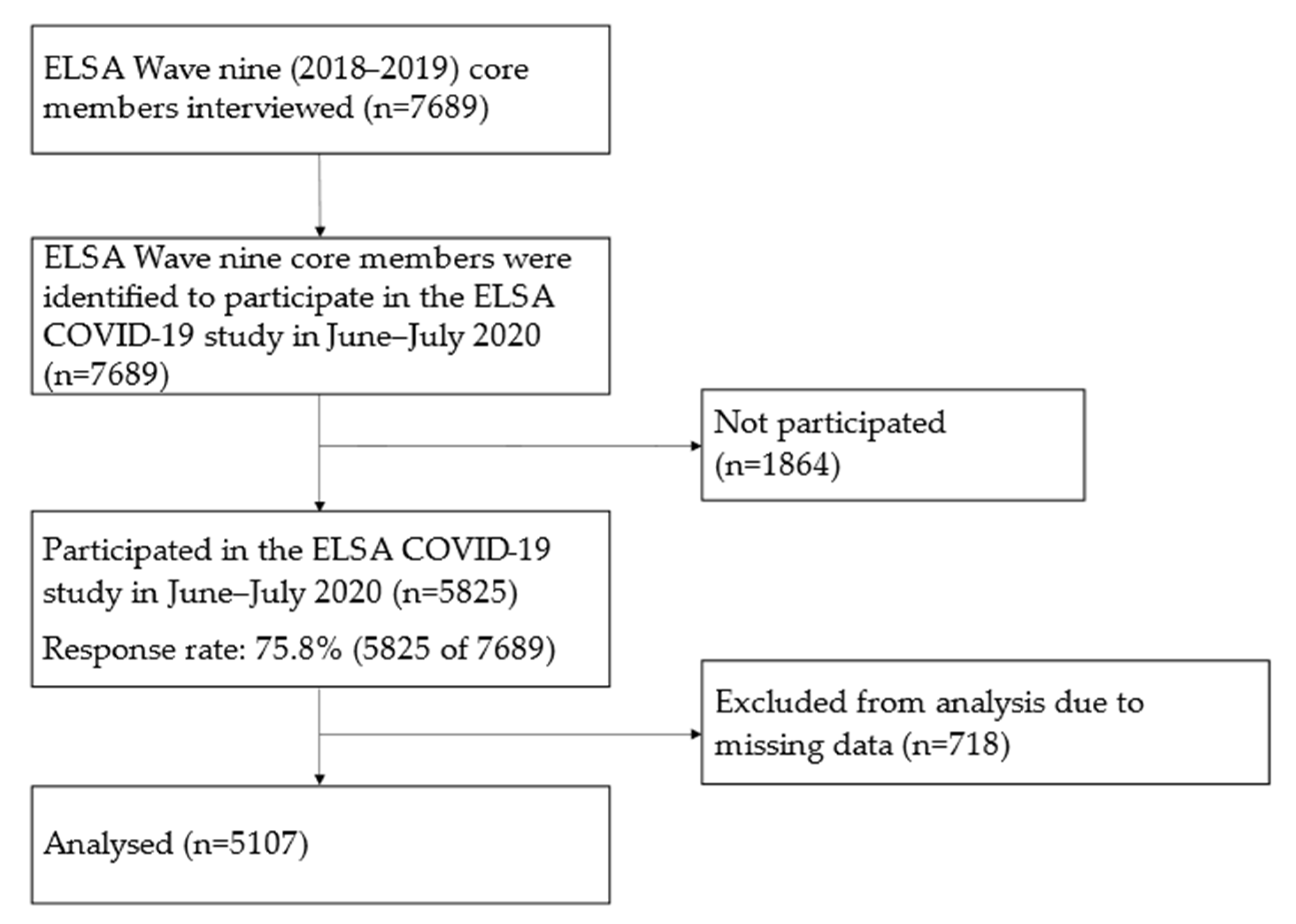
2.1. Study Design and Setting
2.2. Participants
2.3. Measures
2.3.1. Measures from the ELSA COVID-19 Study
2.3.2. Measures from the ELSA Wave Nine
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics and Bivariate Analysis Results
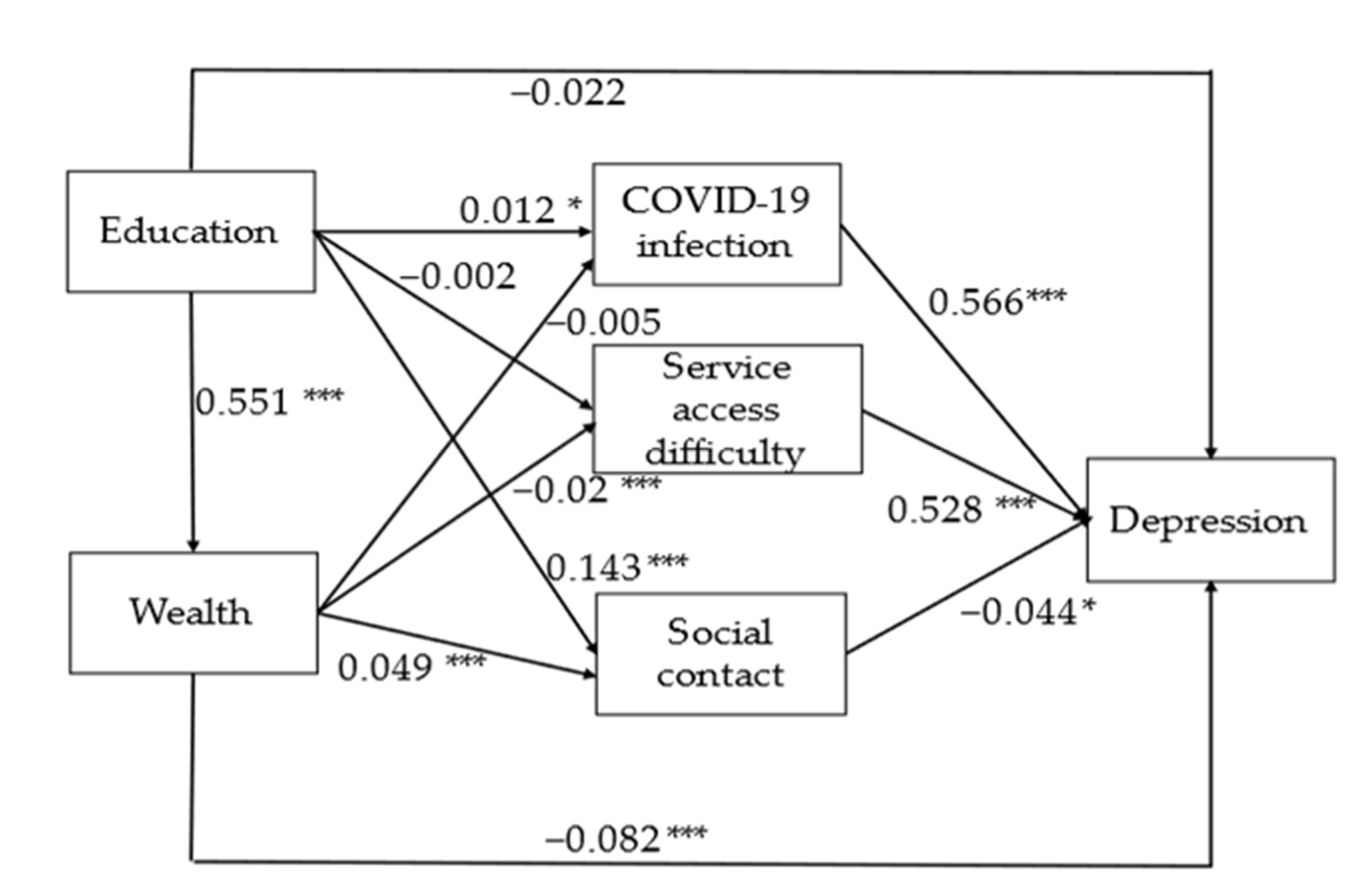
3.2. Path Analysis Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Coefficients (Standard Error) | |
|---|---|
| Education direct effect | −0.036 (0.027) |
| Education > COVID-19 infection | 0.004 (0.003) |
| Education > service access difficulty | −0.003 (0.004) |
| Education > social contact | −0.007 (0.003) * |
| Education > income | −0.03 (0.009) *** |
| Education > income > COVID-19 infection | 0.001 (0.001) |
| Education > income > service access difficulty | −0.004 (0.002) ** |
| Education > income > social contact | −0.001(<0.001) |
| Total indirect effects of education | −0.04 (0.011) *** |
| Total effects of education | −0.076 (0.027) ** |
| Income direct effect | −0.058 (0.016) *** |
| Income > COVID-19 infection | 0.002 (0.002) |
| Income > service access difficulty | −0.009 (0.003) ** |
| Income > social contact | −0.002 (0.001) |
| Total indirect effects of income | −0.008 (0.004) * |
| Total effects of income | −0.066 (0.016) *** |
| Coefficients (Standard Error) | |
|---|---|
| Education direct effect | −0.038 (0.031) |
| Education > COVID-19 infection | 0.008 (0.004) |
| Education > service access difficulty | −0.002 (0.005) |
| Education > social contact | −0.003 (0.003) |
| Education > wealth | −0.042 (0.010) *** |
| Education > wealth > COVID-19 infection | −0.001 (0.001) |
| Education > wealth > service access difficulty | −0.004 (0.002) * |
| Education > wealth > social contact | −0.001 (0.001) |
| Total indirect effects of education | −0.046 (0.011) *** |
| Total effects of education | −0.084 (0.030) *** |
| Wealth direct effect | −0.082 (0.019) *** |
| Wealth > COVID-19 infection | −0.002 (0.002) |
| Wealth > service access difficulty | −0.007 (0.004) * |
| Wealth > social contact | −0.001 (0.002) |
| Total indirect effects of wealth | −0.011 (0.005) * |
| Total effects of wealth | −0.092 (0.019) *** |
| Coefficients (Standard Error) | |
|---|---|
| Education direct effect | 0.006 (0.061) |
| Education > COVID-19 infection | 0.005 (0.008) |
| Education > service access difficulty | 0.004 (0.009) |
| Education > social contact | −0.009 (0.006) |
| Education > wealth | −0.059 (0.019) ** |
| Education > wealth > COVID-19 infection | −0.002 (0.002) |
| Education > wealth > service access difficulty | −0.008 (0.004) * |
| Education > wealth > social contact | 0.002 (0.002) |
| Total indirect effects of education | −0.068 (0.023) ** |
| Total effects of education | −0.062 (0.06) |
| Wealth direct effect | −0.082 (0.019) *** |
| Wealth > COVID-19 infection | −0.004 (0.004) |
| Wealth > service access difficulty | −0.014 (0.006) * |
| Wealth > social contact | 0.003 (0.003) |
| Total indirect effects of wealth | −0.015 (0.008) |
| Total effects of wealth | −0.116 (0.032) *** |
References
- World Health Organization; Calouste Gulbenkian Foundation. Social Determinants of Mental Health; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Campion, J.; Bhugra, D.; Bailey, S.; Marmot, M. Inequality and mental disorders: Opportunities for action. Lancet 2013, 382, 183–184. [Google Scholar] [CrossRef]
- Lund, C.; Breen, A.; Flisher, A.; Kakuma, R.; Corrigall, J.; Joska, J.; Swartz, L.; Patel, V. Poverty and common mental disorders in low and middle income countries: A systematic review. Soc. Sci. Med. 2010, 71, 517–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fryers, T.; Melzer, D.; Jenkins, R.; Brugha, T. The distribution of the common mental disorders: Social inequalities in Europe. Clin. Pract. Epidemiol. Ment. Health 2005, 1, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saraceno, B.; Levav, I.; Kohn, R. The public mental health significance of research on socio-economic factors in schizophrenia and major depression. World Psychiatry 2005, 4, 181–185. [Google Scholar]
- Dohrenwend, B.P.; Levav, I.; Shrout, P.E.; Schwartz, S.; Naveh, G.; Link, B.G.; Skodol, A.E.; Stueve, A. Socioeconomic status and psychiatric disorders: The causation-selection issue. Science 1992, 255, 946–952. [Google Scholar] [CrossRef]
- Marmot, M.; Allen, J.; Goldblatt, P.; Boyce, T.; McNeish, D.; Grady, M.; Geddes, I.; Fair Society, Healthy Lives. The Marmot Review. 2010. Available online: www.ucl.ac.uk/marmotreview (accessed on 20 November 2021).
- Jenkins, R.; Bhugra, D.; Bebbington, P.; Brugha, T.; Farrell, M.; Coid, J.; Fryers, T.; Weich, S.; Singleton, N.; Meltzer, H. Debt, income and mental disorder in the general population. Psychol. Med. 2008, 38, 1485–1493. [Google Scholar] [CrossRef] [Green Version]
- Grundy, E.; Hold, G. The socioeconomic status of older adults: How should we measure it in studies of health inequalities? J. Epidemiol. Community Health 2001, 55, 895–904. [Google Scholar] [CrossRef] [Green Version]
- Demakakos, P.; Biddulph, J.P.; Bobak, M.; Marmot, M.G. Wealth and mortality at older ages: A prospective cohort study. J. Epidemiol. Community Health 2016, 70, 346–353. [Google Scholar] [CrossRef] [Green Version]
- Allwood, L.; Bell, A. COVID-19: Understanding Inequalities in Mental Health during the Pandemic; Centre for Mental Health Briefing: London, UK, 2020. [Google Scholar]
- Blundell, R.; Costa Dias, M.; Joyce, R.; Xu, X.W. COVID-19 and inequalities. Fisc. Stud. 2020, 41, 291–319. [Google Scholar] [CrossRef]
- Flint, A.J.; Bingham, K.S.; Iaboni, A. Effect of COVID19 on the mental health care of older people in Canada. Int. Psychogeriatr. 2020, 32, 1113–1116. [Google Scholar] [CrossRef] [Green Version]
- Falkingham, J.; Evandrou, M.; Qin, M.; Vlachantoni, A. Prospective longitudinal study of ‘Sleepless in Lockdown’: Unpacking differences in sleep loss during the coronavirus pandemic in the UK. BMJ Open 2022, 12, e053094. [Google Scholar] [CrossRef] [PubMed]
- Robb, C.E.; de Jager, C.A.; Ahmadi-Abhari, S.; Giannakopoulou, P.; Udeh-Momoh, C.; McKeand, J.; Price, G.; Car, J.; Majeed, A.; Ward, H.; et al. Associations of social isolation with anxiety and depression during the early COVID-19 pandemic: A survey of older adults in London, UK. Front. Psychiatry 2020, 17, 591120. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. Disparities in the Risk and Outcomes of COVID-19; Public Health England: London, UK, 2020. [Google Scholar]
- Islam, M.S.; Ferdous, M.Z.; Islam, U.S.; Mosaddek, A.S.M.; Potenza, M.N.; Pardhan, S. Treatment, persistent symptoms, and depression in people infected with COVID-19 in Bangladesh. Int. J. Environ. Res. Public Health 2021, 18, 1453. [Google Scholar] [CrossRef] [PubMed]
- Evandrou, M.; Falkingham, J.; Qin, M.; Vlachantoni, A. Older and ‘staying at home’ during lockdown: Informal care receipt during the COVID-19 pandemic amongst people aged 70 and over in the UK. SocArXiv 2020, 1–16. [Google Scholar] [CrossRef]
- Propper, C.; Stokckton, I.; Stoye, G. COVID-19 and Disruptions to the Health and Social Care of Older People in England; The Institute for Fiscal Studies: London, UK, 2020. [Google Scholar]
- ONS. Exploring the UK’s Digital Divide. 2019. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/householdcharacteristics/homeinternetandsocialmediausage/articles/exploringtheuksdigitaldivide/2019-03-04 (accessed on 20 November 2021).
- Pentaris, P.; Willis, P.; Ray, M.; Deusdad, B.; Lonbay, S.; Niemi, M.; Donnelly, S. Older people in the context of COVID-19: A European perspective. J. Gerontol. Soc. Work 2020, 63, 736–742. [Google Scholar] [CrossRef]
- Vahia, I.V.; Jeste, D.V.; Reynolds, C.F. Older Adults and the Mental Health Effects of COVID-19. JAMA 2020, 324, 2253–2254. [Google Scholar] [CrossRef] [PubMed]
- Trabelsi, K.; Ammar, A.; Masmoudi, L.; Boukhris, O.; Chtourou, H.; Bouaziz, B.; Brach, M.; Bentlage, E.; How, D.; Ahmed, M.; et al. Globally altered sleep patterns and physical activity levels by confinement in 5056 individuals: ECLB COVID-19 international online survey. Biol. Sport 2021, 38, 495–506. [Google Scholar] [CrossRef] [PubMed]
- Washif, J.A.; Farooq, A.; Krug, I.; Pyne, D.B.; Verhagen, E.; Taylor, L.; Wong, D.P.; Mujika, I.; Cortis, C.; Haddad, M.; et al. Training during the COVID-19 lockdown: Knowledge, beliefs, and practices of 12,526 athletes from 142 countries and six continents. Sports Med. 2022, 52, 933–948. [Google Scholar] [CrossRef]
- Bambra, C.; Riordan, R.; Ford, J.; Matthews, F. The COVID-19 pandemic and health inequalities. J. Epidemiol. Community Health 2020, 74, 964–968. [Google Scholar] [CrossRef]
- ONS. Coronavirus and Depression in Adults, Great Britain: June 2020; ONS: Newport, UK, 2020. [Google Scholar]
- Steptoe, A.; Di Gessa, G. Mental health and social interactions of older people with physical disabilities in England during the COVID-19 pandemic: A longitudinal cohort study. Lancet Public Health 2021, 6, e365–e373. [Google Scholar] [CrossRef]
- Lorant, V.; Deliège, D.; Eaton, W.; Robert, A.; Philippot, P.; Ansseau, M. Socioeconomic inequalities in depression: A meta-analysis. Am. J. Epidemiol. 2003, 157, 98–112. [Google Scholar] [CrossRef] [Green Version]
- Ettman, C.K.; Abdalla, S.M.; Cohen, G.H.; Sampson, L.; Vivier, P.M.; Galea, S. Prevalence of depression symptoms in US adults before and during the COVID-19 pandemic. JAMA Netw. Open 2020, 3, e2019686. [Google Scholar] [CrossRef] [PubMed]
- Mendez-Lopez, A.; Stuckler, D.; McKee, M.; Semenza, J.C.; Lazarus, J.V. The mental health crisis during the COVID-19 pandemic in older adults and the role of physical distancing interventions and social protection measures in 26 European countries. SSM Popul. Health 2022, 17, 101017. [Google Scholar] [CrossRef] [PubMed]
- Reme, B.; Wörn, J.; Skirbekk, V. Longitudinal evidence on the development of socioeconomic inequalities in mental health due to the COVID-19 pandemic in Norway. Sci. Rep. 2022, 12, 3837. [Google Scholar] [CrossRef] [PubMed]
- Wanberg, C.R.; Csillag, B.; Douglass, R.P.; Zhou, L.; Pollard, M.S. Socioeconomic status and well-being during COVID-19: A resource based examination. J. Appl. Psychol. 2020, 105, 1382–1396. [Google Scholar] [CrossRef] [PubMed]
- Hoebel, J.; Grabka, M.M.; Schröder, C.; Haller, S.; Neuhauser, H.; Wachtler, B.; Schaade, L.; Liebig, S.; Hövener, C.; Zinn, S. Socioeconomic position and SARS-CoV-2 infections: Seroepidemiological findings from a German nationwide dynamic cohort. J. Epidemiol. Community Health 2022, 76, 350–353. [Google Scholar] [CrossRef] [PubMed]
- Syed, S.T.; Gerber, B.S.; Sharp, L.K. Traveling towards disease: Transportation barriers to health care access. J. Community Health 2013, 38, 976–993. [Google Scholar] [CrossRef] [Green Version]
- Ellison, N.B.; Hancock, J.T. Stocking the Social Pantry: A Recipe for Getting from Social Distancing to Distant Socializing. Medium, 8 April 2020. Available online: https://medium.com/@nicoleellison/stocking-the-social-pantry-a-recipe-for-getting-from-social-distancing-to-distant-socializing-6e2a21133858 (accessed on 20 November 2021).
- Seifert, A. The digital exclusion of older adults during the COVID-19 pandemic. J. Gerontol. Soc. Work 2020, 63, 674–676. [Google Scholar] [CrossRef]
- Independent Age. Independent Age Survey Reveals Challenges Faced by Over-65s during Pandemic. 2020. Available online: https://www.independentage.org/newsmedia/press-releases/independent-age-surveyreveals-challenges-faced-by-over-65s-during (accessed on 10 November 2021).
- Banks, J.; Phelps, A.; Oskala, A.; Steptoe, A.; Blake, M.; Oldfield, Z.; Marmot, M.; Clemens, S.; Rogers, N.; Nazroo, J. English Longitudinal Study of Ageing: Waves 0–9, 1998–2019, 35th ed.; [Data Collection], SN: 5050; UK Data Service: Colchester, UK, 2021. [Google Scholar] [CrossRef]
- Steptoe, A.; Addario, G.; Banks, J.; David Batty, G.; Coughlin, K.; Crawford, R.; Dangerfield, P.; Marmot, M.; Nazroo, J.; Oldfield, Z.; et al. English Longitudinal Study of Ageing COVID-19 Study, Waves 1–2, 2nd ed.; [Data Collection], SN: 8688; UK Data Service: Colchester, UK, 2020. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Karim, J.; Weisz, R.; Bibi, Z.; Rehman, S. Validation of the eight-item Center for Epidemiologic Studies Depression Scale (CES-D) among older adults. Curr. Psychol. 2015, 34, 681–692. [Google Scholar] [CrossRef]
- Albert, J.M.; Cho, J.I.K.; Liu, Y.Y.; Nelson, S. Generalized causal mediation and path analysis: Extensions and practical considerations. Stat. Methods Med. Res. 2019, 28, 1793–1807. [Google Scholar] [CrossRef] [PubMed]
- VanderWeele, T.J. Mediation analysis: A practitioner’s guide. Annu. Rev. Public Health 2016, 37, 17–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Mental Health Foundation. The COVID-19 Pandemic, Financial Inequality and Mental Health. 2020. Available online: https://www.mentalhealth.org.uk/sites/default/files/MHF-covid-19-inequality-mental-health-briefing.pdf (accessed on 10 November 2021).
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Healthwatch. Locked Out: Digitally Excluded People’s Experiences of Remote GP Appointments; Healthwatch: Newcastle upon Tyne, UK, 2021. [Google Scholar]
- Alimoradi, Z.; Brostrom, A.; Tsang, H.W.H.; Griffiths, M.D.; Haghayegh, S.; Ohayon, M.M.; Lin, C.; Pakpour, A.H. Sleep problems during COVID-19 pandemic and its’ association to psychological distress: A systematic review and meta-analysis. ECLinicalMedicine 2021, 36, 100916. [Google Scholar] [CrossRef]
- Cabinet Office Guidance COVID-19 Response: Living with COVID-19. Updated 23 February 2022. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1056229/COVID-19_Response_-_Living_with_COVID-19.pdf (accessed on 10 April 2022).
- Age UK. Digital Inclusion and Older People—How Have Things Changed in a COVID-19 World? Age UK: London, UK, 2021. [Google Scholar]
| Number (% among All Respondents) | Row % of Depression Caseness | p Value | |
|---|---|---|---|
| All respondents | 5107 (100.0) | 19.7 | |
| Age | Mean age of all respondents 67.1 | Mean age of depressed 66.4; Mean age of not depressed 67.2 | 0.026 |
| Gender | <0.001 | ||
| Male | 2211 (47.2) | 14.5 | |
| Female | 2896 (52.8) | 24.4 | |
| Education | <0.001 | ||
| Less than O-level or equivalent | 1283 (30.0) | 23.8 | |
| O-level or equivalent | 1721 (35.2) | 20.2 | |
| A-level or higher | 2103 (34.8) | 15.8 | |
| Household wealth quintile | <0.001 | ||
| Lowest | 683 (20.1) | 31.4 | |
| 2 | 869 (19.2) | 22.9 | |
| 3 | 1145 (21.0) | 17.3 | |
| 4 | 1208 (20.3) | 13.6 | |
| Highest | 1202 (19.4) | 13.6 | |
| Two or more core COVID-19 symptoms | <0.001 | ||
| No | 4514 (87.0) | 16.8 | |
| Yes | 593 (13.0) | 39.1 | |
| Difficulty in accessing services | <0.001 | ||
| No | 3658 (71.8) | 14.1 | |
| Yes | 1449 (28.2) | 34.2 | |
| Social contact score | 0.002 | ||
| 0 | 172 (3.9) | 27.7 | |
| 1 | 314 (6.2) | 25.2 | |
| 2 | 942 (19.4) | 20.6 | |
| 3 | 688 (13.5) | 18.8 | |
| 4 | 2991 (57.0) | 18.5 | |
| Pre-pandemic depression | <0.001 | ||
| No | 4574 (87.4) | 13.8 | |
| Yes | 533 (12.6) | 60.6 |
| Coefficients (Standard Error) | |
|---|---|
| Education direct effect | −0.022 (0.027) |
| Education > COVID-19 infection | 0.007 (0.004) * |
| Education > service access difficulty | −0.001 (0.004) |
| Education > social contact | −0.006 (0.003) * |
| Education > wealth | −0.045 (0.009) *** |
| Education > wealth > COVID-19 infection | −0.002 (0.001) |
| Education > wealth > service access difficulty | −0.006 (0.002) ** |
| Education > wealth > social contact | −0.001 (0.001) |
| Total indirect effects of education | −0.054 (0.011) *** |
| Total effects of education | −0.076 (0.027) ** |
| Wealth direct effects | −0.083 (0.017) *** |
| Wealth > COVID-19 infection | −0.003 (0.002) |
| Wealth > service access difficulty | −0.010 (0.003) ** |
| Wealth > social contact | −0.002 (0.001) * |
| Total indirect effects of wealth | −0.015 (0.004) *** |
| Total effects of wealth | −0.098 (0.017) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qin, M.; Evandrou, M.; Falkingham, J.; Vlachantoni, A. Did the Socio-Economic Gradient in Depression in Later-Life Deteriorate or Weaken during the COVID-19 Pandemic? New Evidence from England Using Path Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6700. https://doi.org/10.3390/ijerph19116700
Qin M, Evandrou M, Falkingham J, Vlachantoni A. Did the Socio-Economic Gradient in Depression in Later-Life Deteriorate or Weaken during the COVID-19 Pandemic? New Evidence from England Using Path Analysis. International Journal of Environmental Research and Public Health. 2022; 19(11):6700. https://doi.org/10.3390/ijerph19116700
Chicago/Turabian StyleQin, Min, Maria Evandrou, Jane Falkingham, and Athina Vlachantoni. 2022. "Did the Socio-Economic Gradient in Depression in Later-Life Deteriorate or Weaken during the COVID-19 Pandemic? New Evidence from England Using Path Analysis" International Journal of Environmental Research and Public Health 19, no. 11: 6700. https://doi.org/10.3390/ijerph19116700
APA StyleQin, M., Evandrou, M., Falkingham, J., & Vlachantoni, A. (2022). Did the Socio-Economic Gradient in Depression in Later-Life Deteriorate or Weaken during the COVID-19 Pandemic? New Evidence from England Using Path Analysis. International Journal of Environmental Research and Public Health, 19(11), 6700. https://doi.org/10.3390/ijerph19116700